MissingSchool made a public submission in response to the Commonwealth Department of Education’s consultation.
2025 Review of the Disability Standards for Education
This submission responds to the 2025 Review of the Disability Standards for Education (DSE).
Its purpose is to:
- present experiences of students with chronic medical-mental illness and absence;
- demonstrate where implementation of the DSE currently falls short for this cohort; and
- propose strengthened, contemporary standards under Topics 1, 2 and 3 to ensure adjustments for access, continuity, and participation for these students is on the same basis.
MissingSchool makes this submission as a specialist organisation in this area.
About MissingSchool
Specialist Organisation for Students with Chronic Medical and Mental Illness.
Founded in 2012, MissingSchool is dedicated to ending school isolation for K–12 students experiencing chronic medical and mental illness and extended absence.
We partner with schools, families, clinicians, and policymakers to design system solutions that keep students connected to their learning and school communities when they can’t physically attend.
Our mission is to build national school capability for “learn-from-anywhere” telepresence so students remain present—academically, socially, and emotionally—from all places of care.
Our advocacy has catalysed public understanding of this hidden cohort, with 450+ media stories and a national campaign that has reached over 14.1 million Australians.
National Reach and Evidence Base
Operates a data-driven service model for national evidence on chronic illness-related absence.
Service outcomes since 2018 through ~8,000+ direct interactions with families and schools annually:
- 7,770 classmates reconnected through telepresence placements.
- 3,360 teachers engaged/trained, building practical inclusion capability.
- 989 surveys and 626 long-form interviews from students, parents, teachers, and clinicians.
- 8,675 qualitative evidence points thematically coded in our national database.
- Engaging a national alliance of over 38 health consumer organisations and supported by a directory of 250+ health and children’s organisations strengthening advocacy.
The evidence in this submission supports telepresence as a workable, scalable, equitable DSE practice that keeps students connected to school and bridges their return to physical attendance.
Tasmania (DECYP) will trial school-led videoconferencing solutions to increase attendance in 2025.
Why Adjust for Attendance
Unlike hospital school or distance education—which don’t keep students connected to their regular schools—telepresence provides real-time access to the student’s actual classroom. It:
- preserves student identity, belonging, and peer connection;
- reduces learning gaps;
- maintains teacher-student relationships;
- creates “teach once” efficiencies; and
- significantly improves student reintegration.
Families and teachers consistently report increases in confidence, social participation, wellbeing, engagement, and—critically—we see an increase in attendance for around 50% of students that accessed their classroom via telepresence.
Telepresence demonstrates: the solution to absence is not attendance—it is presence.
The Students Behind the Data
Student context*
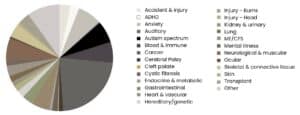
*Note this graph represents conditions experienced by students engaged with MissingSchool and is not representative of all possible conditions students may experience or their distribution.
Illness-related absence is not marginal. Up to one in three (1.2 million) Australian students miss significant periods of school each year due to chronic medical or mental illness.
Almost 40% of students we support have missed seven months or more and more than 50% expect to miss another 7+ months. Absence patterns are dominated by indefinite and intermittent illness, not short-term disruptions.
Our service demographics—1% non-binary; 5% Aboriginal and Torres Strait Islander; 43% female; 56% male— are representative of the need for policies inclusive of diverse student populations. 87% of the students we support have siblings and 28% of those siblings also miss school.
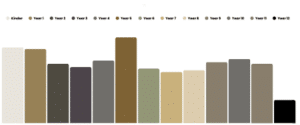
Students by school age
Before telepresence, many had little or no access to learning:
- 25% received no support at all
- 37% accessed hospital schools
- 50% had work packets sent home to do alone
- Only 15% had any digital connection
In line with the literature, parents report that students face disrupted relationships (71%), diminished academic achievement (55%), increased anxiety (54%), reduced social support (50%) and developmental delays (39%).
These gaps represent systemic inequity, not student choice.
Bullying, exclusion, and academic impact
Students with chronic medical and mental illness face:
- far higher bullying rates—up to five times higher rates of bullying than peers;
- greater social isolation, poorer wellbeing, and weaker reintegration;
- higher likelihood of falling below NAPLAN minimum standards; and
- long-term risks to school completion, employment, and wellbeing.
For the most severely unwell students—those hospitalised repeatedly—up to 40% did not sit NAPLAN at all, while those who did were 30–60% more likely not to meet minimum standards.
40% of students in Australia who do not complete year 12 have a chronic illness.
Illness impacts learning because illness impacts access.
Schools Supporting Students Through Telepresence
MissingSchool has placed telepresence technologies in 215 schools across all states and territories, spanning the socio-educational spectrum:
- Government (≈66%), Catholic, and Independent sectors
- Schools ranging from 21 students to 3,000+
- Strongest engagement in NSW and Tasmania
- Schools representing 135,996 students and 16,230 teachers
Schools engaged by state
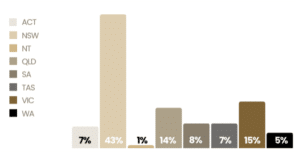
Telepresence has been used in schools with high, mid, and low ICSEA scores, confirming it as a universal inclusion tool—not tied to geography, funding level, or advantage.
Yet, only 39% of students have an Individual Education Plan, despite clear DSE entitlements.
This reflects a systemic misunderstanding that illness is covered by the DSE—and a pressing need for applications of the Standards that speak directly to this under-supported cohort.
Why the DSE Matters—And Why It Needs Strengthening
The Disability Standards for Education set out essential provisions:
- Accessible, non-discriminatory education for all students with disability.
- A broad definition of disability—including medical illness, mental illness, imputed illness.
- Entitlements to enrolment, participation, curriculum, support services, protection from harassment, reasonable adjustments, and coordinated services.
- Prohibition of gatekeeping; and no segregating students to non-mainstream education.
- Requirements for schools to provide equitable access and continuity of curriculum.
Despite provisions, illness-related absence remains systematically under-recognised and either inconsistently supported, or not supported at all, leaving many students without continuous access to learning, peers, and community.
This Review provides a critical opportunity to modernise the DSE to reflect contemporary learning environments, digital access, and the real-world needs of students with chronic illness.
Responses to Topics 1, 2 and 3
This submission draws on MissingSchool’s national evidence and lived experience to address three themes central to this Review:
Topic 1 — Recognition – Ensuring illness and complex absence are fully and explicitly recognised as forms of disability requiring reasonable adjustments—including remote access.
Topic 2 — Access, Participation – Embedding minimum standards for continuity of learning, digital access, telepresence, and strengthening protections for students disproportionately victimised.
Topic 3 — Harassment & Victimisation – Strengthening continuity for students disproportionately neglected due to illness, and making social and academic participation portable.
| Student Story
A student from ACT with a long-term, complex illness has experienced substantial school absence since early primary years. Early disengagement led to significant learning gaps, reflected in low Year 3 NAPLAN performance and delays across literacy, numeracy, and language by Year 5. He frequently received ‘Status’ grades due to insufficient evidence of progress. Following referral in 2021, the student received a telepresence device, enabling full participation in classroom teaching despite extended hospitalisations. Over two years he was physically absent for 246 days but able to attend all lessons in real time. In the current year, just 37% of his schooling has been onsite, with the remaining 63% completed remotely through the robot. The continuity provided by telepresence has resulted in measurable academic improvement: a consistent B-average, age-appropriate literacy and numeracy, and strengthened engagement with peers and school life. During a recent two-week, interstate hospital stay, he completed two mathematics exams via school telepresence and now ranks first in science and second in mathematics and geography. This case highlights how reliable access to telepresence technology—supported by school-based inclusion teams—can prevent irreversible learning loss, maintain assessment participation, and enable high achievement for students experiencing chronic medical illness and absence. It is not the illness, nor the absence, but the access that matters. |
Background
In Australia, students with chronic medical and mental illness and absence are falling through an equity gap. Medical illness remains under-recognised under the DSE, and schools often misapply the Standards by deciding which illnesses they will acknowledge, including when directing students to or accepting students into distance education due to chronic non-attendance.
The DSE’s definition of illness disability is broad—it does not require permanency, diagnosis, visible evidence, or certainty, and it explicitly supports imputed disability or effects of past illness.
Gatekeeping practices—such as denying videoconferencing as a reasonable adjustment—block access to classrooms, curriculum, peers, and support during unavoidable absence, pushing families into distance education or homeschooling, which still rely on online learning to access education.
Segregation from regulated mainstream schooling—to unregulated environments—undermine education access, equity, quality, and child safety, enabling unacceptable outcomes.
Topic 1: Knowing about and using the Standards (effective implementation)
| A Year 10 student from New South Wales has missed more than two years of school due to ME/CFS and anxiety. She is a gifted and enthusiastic student who now only manages brief study sessions when her health allows. Despite strong support from her school, system limitations have left her without education continuity. She was denied permission to record classes because the school would not accept a camera in the classroom, and she was regarded ineligible for distance education. Worksheets replaced teaching, causing total disconnection from learning and peers, academic loss and deep social isolation.
Parent: “We spent four months trying to sort out engagement with Distance Education. Then they changed their minds and said [child] didn’t fit the criteria, along with 100 other students across the state. This is a loophole to not back certain students who are “too difficult”. Went back to the high school. Microsoft Teams was the solution, but this was done poorly. For maths, worksheets were put online, but there was no learning or explanation attached, and then we’re not knowing where to go to get the teaching aspect. The GP considered admitting her to hospital, just so they may be eligible for hospital school education/services.” |
“I work in student wellbeing in regional NSW. I’m struggling to access support for students with disabilities. A student with chronic anxiety and autism can’t attend full-time school due to noise and change, missing teacher interaction and support.” ~ Teacher
The DSE regulates for equal access to education for students with medical and mental illness (or imputed illness before diagnosis), regulating schools to make reasonable adjustments, including for health-absences. Recommendation 1: Strengthen DSE recognition for students with medical and mental illness (including imputed illness before diagnosis) as eligible for reasonable adjustments.
“We were told to return to Distance Ed. Tried reducing to 3 classes a week, but they insisted on full-time. [Student] was in tears. He’ll do grades 7-9 in distance ed, then hopefully return for 10-12 but we’re still enrolling—why couldn’t he finish the year at his school?” ~ Parent
Schools must not decide which illnesses are recognised and should distinguish between the NDIS, which requires permanent disability, and the DSE, which does not. The DSE supports invisible illness and imputation. Differential/discriminatory definitions (NDIS, Thriving Kids, DSE) need alignment. Recommendation 2: Clarify that schools cannot determine which illnesses are “acceptable.” Unlike the NDIS, the DSE does not require permanency, diagnosis, or visibility of illness.
“[Student] has struggled with kidney issues since year five, missing school and not catching up on work as teachers didn’t require it. By year eight, they had no friends, was tired from frequent hospital visits, and faced challenges with learning and socialising.” ~ Teacher
The Nationally Consistent Collection of Data (NCCD) website confirms the DSE covers students who care for someone with a disability, but this important interpretation is largely unknown, leaving many young carers and siblings overlooked by their schools for support. Recommendation 3: Make the DSE’s coverage of young carers explicit in Standards guidance, training, and school obligations.
“[Student’s] school hasn’t addressed his part-time needs. Fatigue limits work at home, and invisible symptoms make it hard to prove his needs. Chronic Fatigue Syndrome doesn’t qualify for at-home support, and he wasn’t ‘sick enough’ for extra help or a teacher’s aide.” ~Parent
A cold is not the same as cancer or chronic anxiety. A new “chronic illness” code within the approved absence category would enable early detection of chronic absence and trigger DSE reasonable adjustments. Recommendation 4: Introduce a “chronic illness”absence code to enable early detection and trigger reasonable adjustments.
The student’s complex health needs have led to school refusal, compounded by anxiety from extended absences. Frequent appointments and feeling unwell make it difficult for their carer to get them to school consistently.” ~ Teacher
An undiagnosed condition is not truancy or bad behaviour. An illness can be “imputed” through the DSE, without formal diagnosis, based on symptoms/circumstances (including repeat absences) for DSE support. Recommendation 5: Promote early support for undiagnosed conditions by recognising illness imputation based on symptoms or repeated absence.
“We had to move my child’s school due to ongoing bullying over their cancer and mobility issues. The teachers were neither aware nor supportive, making it a difficult situation.” ~ Parent
The DSE seeks protection from stigma and exclusion for students living with illness. That is only as strong as a school’s application of the DSE, which is currently systemically lacking (particularly for invisible illness). Recommendation 6: Strengthen accountability for protecting students with illness from stigma and exclusion, including those with invisible illness.
“For the student, their class felt out of sight, out of mind for them. They needed support for mental wellbeing and counselling, as their mood affected both them and others. Accessing available support is crucial in such situations.” ~Teacher
The DSE does not limit equality to physical presence, signalling that students who have chronic absence due to illness still have a right to access their schools with assistive devices and to receive ongoing support. Recommendation 7: Affirm that DSE extends beyond physical school attendance—students with chronic illness and absence can access school attendance using assistive technology.
“The student accesses online work but misses the teaching part. With a reduced curriculum and limited support, they’re trying to catch up. Their erratic attendance makes extra support hard, and they need a reliable way to learn from home when in pain.” ~ Parent
COVID-19 confirms schools’ and technology’s role in continuing education for students homebound in a health crisis (amend B.3.6 NCCD Guidelines to recognise learning from home as an eligible adjustment, enabling assistive videoconferencing technology for classroom and curriculum access, learning alongside peers). Recommendation 8: Amend NCCD Guidelines (B.3.6) to recognise learning from home as an eligible adjustment, enabling assistive videoconferencing for classroom and curriculum access alongside peers.
“The student completed 2.5 years of leukaemia treatment but now faces more hospitalisation and limited time with family and friends. Connection methods can reduce stress and support relationships with peers and the school community.” ~ Teacher
Videoconferencing to classes, and targeted school tutoring across home, hospital, and school would provide learning continuity alongside peers, and specialised support, while NCCD tracking would help close Australia’s data gap. Recommendation 9: Implement classroom videoconferencing and targeted school tutoring across home, hospital, and school settings to sustain learning continuity and peer connection, so NCCD tracking helps close Australia’s data gap, and schools get funding levy.
Topic 2 – Inclusive decision making and complaints handling
| A Year 9 student from Queensland lives with Autism, ADHD, anxiety, and complex medical needs, often moving between school, home and hospital settings for treatment and recovery. A fun-loving student who likes jokes, she enjoys writing stories, dancing and playing with her dog. After recent medical treatment, her school attendance has become intermittent and uncertain. While her school provides work to complete at home, lessons often rely on self-direction, which has increased her anxiety. She was refused video participation as it was not “approved”, leaving few alternatives for meaningful inclusion.
Parent: “I was gutted and met with complete resistance from (school). They said, ‘nowhere has it been approved other than a rural school where everyone knows each other and people are ok with it being a video.’ So, I asked ‘what would you come to the table with?’ They gave me nothing. I asked ‘How can you help? What can you do to help me with this situation?’ I didn’t get anything. Finally, they said for some programs like maths, they can give [Child] access to the same program at home. Finally, that was something at least. That’s coming to the table.” This demonstrates how rigid systems, and unclear processes hinder school responsibility. |
“I guess I was caught off guard when the school said ‘no’ [to use of technology for reasonable adjustments]. I hadn’t considered that anybody would say ‘no’. I don’t understand why they would say ‘no’.” ~Parent
Families, students, and clinicians must be included in multidisciplinary decision-making to ensure adjustments reflect medical, educational, and wellbeing needs, including before chronic absence affects school access and increases anxiety for return. Recommendation 10: Embed multidisciplinary collaboration with families, students, and clinicians in adjustment planning to ensure medical, educational, and wellbeing needs are met before chronic absence sets in.
“[Student] would often be absent for weeks due to their health, making it hard to maintain relationships and leaving them feeling excluded. They couldn’t participate in many activities, even if they were at school.” Teacher
Schools need clear guidance to provide ongoing, adaptive adjustments that are portable across all stages of schooling, transitions between years and schools, and other places of care (home, hospital/clinical settings). Recommendation 11: Establish clear systems and processes for schools to provide ongoing, adaptive adjustments, that are portable across all schooling stages, transitions, and care settings (home, hospital, clinic).
“We are struggling to know exactly how to support him as he feels he is getting further and further behind. His school are limited in their capacity to assist.” ~Parent
Require an education provider to follow included principles when they consult, resolve issues or handle complaints arising in relation to the DSE and a student or prospective student; no ambiguity. Recommendation 12: Define decision-making and complaints-handling processes, including escalation pathways for families, within the DSE or guidelines to better support students, eliminate ambiguity, strengthen school accountability.
Topic 3 – Clear responsibilities for assessment/course authorities/ developers
| A Year 12 student from Western Australia, undergoing treatment for cancer, was absent from school for most of the year and expected to remain away indefinitely. His hands-on VET industry program is impossible to access from medical isolation. ADHD makes focus challenging, yet he is highly engaged when learning aligns with his interests.
Despite strong support from his school, major gaps in planning and adjustments left him without a meaningful education pathway. He was not provided with an Individual Education Plan and was told early on that he would not complete Year 12—only a Certificate I—because his practical coursework could not be adapted. Hospital school offered some learning, but not the specialised VET content he needed. Long-standing bullying at his previous school and the family’s 40km distance from campus further compounded his social isolation.
The consequences have been clear: disrupted learning, rising anxiety, attention challenges, and weakened peer relationships. Friends struggle to stay in touch due to hospital internet issues and their own limited access to technology, leaving him disconnected when he most needs support.
Telepresence technology was eventually introduced, offering a pathway back into classes and peer life, but delays, resistance, and technical hurdles meant months of lost connection. His experience shows how slow decision-making, unclear responsibilities, and limited understanding of the Disability Standards for Education can leave students with serious health conditions without continuity, belonging, or appropriate adjustments, even when solutions exist. |
“There is no plan. The learning support teachers meet with him, and they show him how to set up a study plan to catch up on work, but they haven’t been much help. In fact, they have been threatening that he needs 85% attendance to comply with NESA, or he will get a warning letter, and he will have to leave school.” ~ Parent
Families carry the burden of coordination and advocacy, repeatedly justifying with documentation and explaining their child’s medical and mental illness (including absences) across agencies and settings. Recommendation 13: Reduce administrative burden and punitive measures placed on families by streamlining documentation and coordination across agencies and systems.
“The challenge is with horticulture, as it’s practical and involves being outdoors, which isn’t ideal. For subjects like PE or horticulture, where students are planting, pulling weeds, or doing cuttings, I don’t have a practical solution for that.” ~ Teacher
Co-designed adjustments – including videoconferencing for class access counted as attendance – must be health-informed, accommodating fluctuating absences, fatigue, symptoms/effects of medication/treatment. Recommendation 14: Require co-designed, health-informed adjustments that accommodate fluctuating absence, fatigue, medication effects, and home and hospital stays—with class videoconferencing counted as attendance.
“Some teachers send work, but others don’t. The school isn’t adjusting assessments to match where the student is or their abilities. After asking for support, they said it depended on their subject choices. We’ve made those, but haven’t received any follow-up.” ~ Parent
Education authorities must make adjustments portable so they follow students across all settings/situations (learning from home, hospital, exams, training, assessment, placements) and transitions, for continuity and equity. Recommendation 15: Mandate portability of adjustments across all learning settings, including learning from home, hospital, exams, training, placements, and transitions, ensuring continuity and equity across time, places, and activities.
Conclusion
The 2025 Review of the Disability Standards for Education is a rare chance to correct a long-standing blind spot in Australian education. Students with chronic medical and mental illness are not on the margins of the system—they are in every classroom, on every roll, and too often left without continuous access to learning, peers, and future opportunities.
The evidence in this submission shows that when the DSE is properly understood and applied—when illness is explicitly recognised, reasonable adjustments include remote access, and responsibilities are clear—students not only stay connected, they succeed.
Telepresence and school-led videoconferencing are not “nice-to-have” extras; they are contemporary, workable expressions of the DSE’s core promise of equal access. We urge this Review to make that promise real: by acknowledging illness, embedding digital access and portability of adjustments, closing data gaps, and strengthening accountability so no student is exiled from their own education or school because they have a physical or mental illness that causes unavoidable absence.
It is not absence that defines these students’ lives, but whether we guarantee their presence.